SUMMARY
The principle of wastewater diagnostics is a suitable complementary approach that can help to gain epidemiological information on a large part of the population in a non-invasive way. The course of the pandemic spread of the new coronavirus (SARS-CoV-2) has been showing a cyclical course of successive waves of Covid-19 since 2020. For this model, a systematic detection of the occurrence of its agent in wastewater is a very effective approach.
In our study, the coronavirus SARS-CoV-2 was monitored in wastewater from selected wastewater treatment plants (WWTP) in the Czech Republic between April 2020 and January 2022. Current findings and conclusions of ongoing studies have clearly shown that, in its targeted and systematic implementation, wastewater monitoring can be a suitable complement to epidemiological forecasts, proposals for measures, and thus the protection of public health. In addition, our results showed that WWTP of all categories are suitable for epidemiological diagnostics of wastewater. However, in a systematic epidemiological approach to wastewater (“Wastewater-Based Epidemiology”; WBE), it will be necessary to consistently accept differences between the types and purposes of monitoring, the nature of wastewater, and the specifics of sampling points.
INTRODUCTION
Wastewater is a recipient of all waste substances and metabolic products excreted by humans. Provided that they do not decompose, these substances are detectable using appropriate methods. This also applies to pathogenic agents and other specific markers which detection in wastewater is one of the goals of wastewater diagnostics. The purpose is to obtain information about the studied population or a specific community. This alternative approach, which uses wastewater as a collective diagnostic medium, currently helps to eradicate polio (poliomyelitis). This infectious disease has been eliminated on some continents, but worldwide vaccination is still needed. In the Czech Republic, polio was completely eradicated in 1961 [1]. Investigation of polioviruses in wastewater in eight cities and refugee camps in the Czech Republic is currently underway according to WHO guidelines within the global polio eradication programme [2]. In non-medical fields, wastewater is used to determine lifestyle markers (drugs and other addictive substances, personal care products, medicines, etc.), both globally and in problematic regions.
Shortly after the outbreak of the Covid-19 pandemic, it became clear that outbreaks could not be monitored effectively enough using current epidemiological approaches, in which infected individuals are identified on the basis of clinical manifestations. The course of the pandemic spread of the coronavirus SARS-CoV-2 has shown a cyclical course of successive waves of Covid-19 since 2020. To implement effective measures to combat the epidemic, using WBE is appropriate. There are currently 3,166 WWTP in the Czech Republic, which makes it possible to keep for about 80% of its population under surveillance [3].
In environmental samples, such as wastewater, there is a presumption of the occurrence of the monitored agents even in very low concentrations. Therefore, it is appropriate to use a larger amount of sample for the analysis itself and to perform a step before isolating the nucleic acids which will allow the concentration of the given agents, in our case viruses. However, this procedure can be a source of increased number of errors, so each step of the analysis must be strictly monitored.
METHODOLOGY
Wastewater sampling from WWTP started in April 2020 and is planned until April 2022. Samples were taken from 66 WWTP of different sizes in different time regimes. In this paper, we present the results of eight selected WWTP with different numbers of connected inhabitants (CI) between April 2020 and January 2022: Buchlovice (2,340 CI); Slavkov u Brna (6,500 CI); Tišnov (11,500 CI); Přerov (41,000 CI); Kladno (80,000 CI); Brno (about 426,000 CI) and Prague Central WWTP (CWWTP) NWL (new water line) and EWL (existing water line), both about 600,000 CI.
In the initial stages, different sampling methods were used depending on current possibilities. Gradually, sampling was optimized to ensure the most representative samples possible. Time experiments were performed, when a series of 24 composite hourly samples (mixed four volume-identical samples taken every 15 min) obtained during 24 hours at the Brno WWTP were taken. In addition to SARS-CoV-2 RNA, selected chemical and physico-chemical parameters were determined in the samples (COD-Cr, N-NH4, o-PO4, suspended solids, faecal coliform bacteria, and enterococci). These experiments showed that the most concentrated wastewater at the WWTP is between 5 a. m. and 11 p. m. Based on this finding, wastewater sampling was tested at shorter intervals (15 min) in the above-mentioned time period and compared with the common 24-hour sampling [4].
In the current stage of sampling, composite 24-hour samples of untreated wastewater were taken using automatic samplers after rough mechanical pre-treatment (screening). Samples were stored refrigerated and processed within 48 hours of collection or frozen at −70 °C.
Detection of SARS-CoV-2 virus in wastewater
The research laboratories of Veterinary Research Institute (VRI) Brno and TGM WRI cooperated to create a methodological procedure for wastewater analysis which includes a precisely defined system of control points to ensure a proper and valid analysis of each sample. These points include:
- Check of wastewater sampling, including samples transport to analytical laboratories under appropriate conditions (ideally: cooled to 3 ± 2 °C, within 48 hours).
- Wastewater treatment check, i. e., concentrating the viral particles from a defined sample volume and subsequently isolating the nucleic acids. This external check of the analysis also makes it possible to determine the efficiency of the whole procedure, which guarantees a more accurate quantification of SARS-CoV-2 (genomic equivalents (GE)) in the monitored samples.
- Check of the course of the SARS-CoV-2 (GE) detection and quantification step in the monitored samples using real-time reverse transcription polymerase chain reaction (RT-qPCR).
This method, which has been approved by the Ministry of Health [5], consists of concentrating a 500 ml sample of wastewater using polyethylene glycol (PEG) and sodium chloride. The commercially available QIAamp Viral RNA Mini Kit (Qiagen, Germany) is used for RNA isolation; moreover, RNA isolation can be fully automated. Quantitative RNA detection of SARS-CoV-2 virus is performed by RT-qPCR method targeted at three independent detection targets in the virus genome (two N gene targets and an area coding non-structural protein nsp12). The sensitivity (detection limit) of the entire methodological procedure (i. e. from the initial concentration of the wastewater sample to the actual quantification of GE SARS-CoV-2) is 2.5 viral particles (GE) in 1 ml of wastewater; the average efficiency of the procedure is 36%. The analyses were performed in the laboratories of VRI Brno and the Brno branch of TGM WRI.
Data evaluation
The obtained data were correlated with the number of people tested positive for Covid-19 in the monitored regions, i. e. cities and municipalities connected to the relevant WWTP. Epidemiological data were obtained from the Department of Biostatistics of the National Institute of Public Health (NIPH) from the national Information System of Infectious Diseases (ISID). People 10 days before the date of the first symptoms until the 3rd day after the positive PCR test (the 14-day interval) were included in the evaluation. Public data obtained from covid maps, which draw data from open data sets of the Ministry of Health, were used for preliminary evaluations. These data are often affected by error and do not include the number of inhabitants in smaller connected municipalities.
RESULTS AND DISCUSSIONS
Within the study, eight WWTP of different size categories were selected from a total of 66 WWTP, ranging from WWTP with 2,340 connected inhabitants (CI) to two water lines of Prague CWWTP with more than 600,000 connected inhabitants. These WWTP were used to evaluate the applicability of the chosen approach to predict disease trends and detect the possible onset of the epidemic. The selected WWTP also differed in the nature of the supplied wastewater. Comparisons of the number of SARS-CoV-2 GE in frozen samples of untreated wastewater and the number of positively tested people at selected WWTP are shown in Fig. 1 to 8.
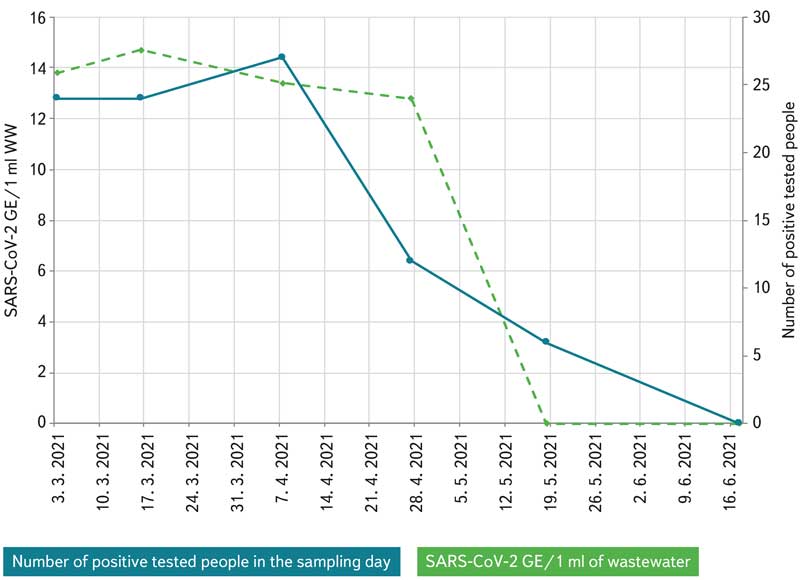
Fig. 1. Comparison of numbers of positive tested persons and amount of GE SARS-CoV-2 in wastewater from Buchlovice WWTP (2,340 connected people)
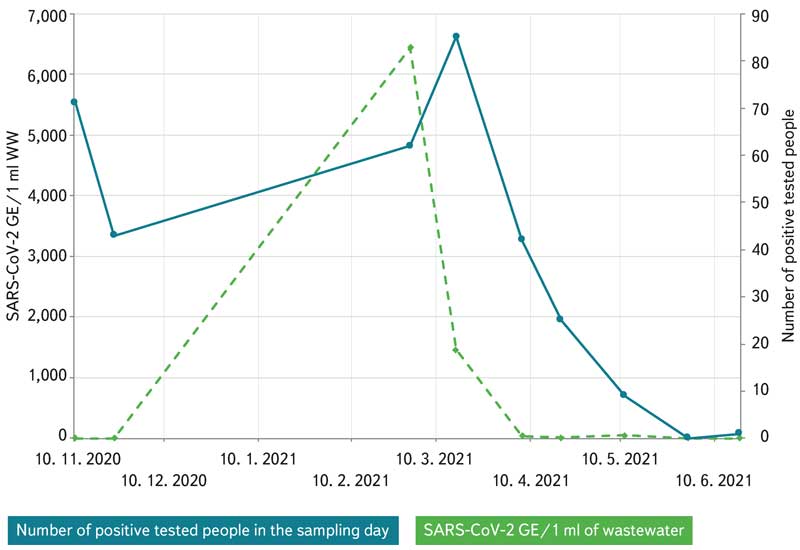
Fig. 2. Comparison of numbers of positive tested persons and amount of GE SARS-CoV-2 in wastewater from Slavkov u Brna WWTP (6,500 connected people)
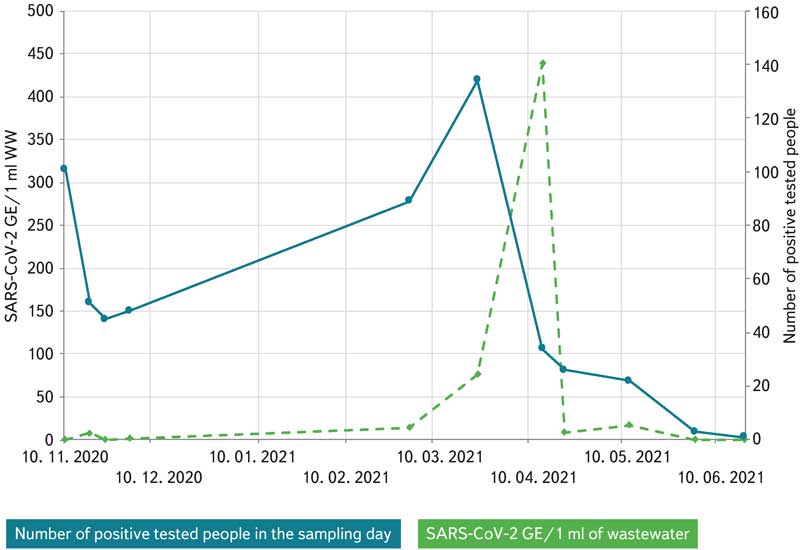
Fig. 3. Comparison of numbers of positive tested persons and amount of GE SARS-CoV-2 in wastewater from Tišnov WWTP (11,500 connected people)
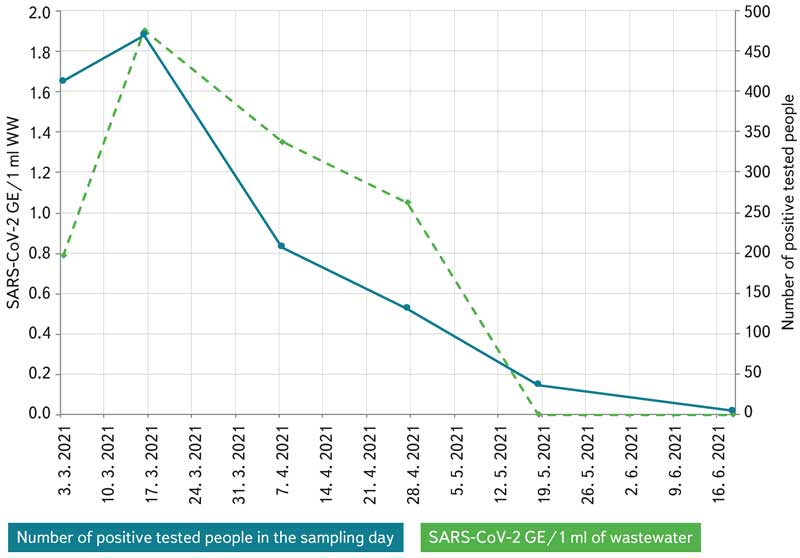
Fig. 4. Comparison of numbers of positive tested persons and amount of GE SARS-CoV-2 in wastewater from Přerov WWTP (41,000 connected people)
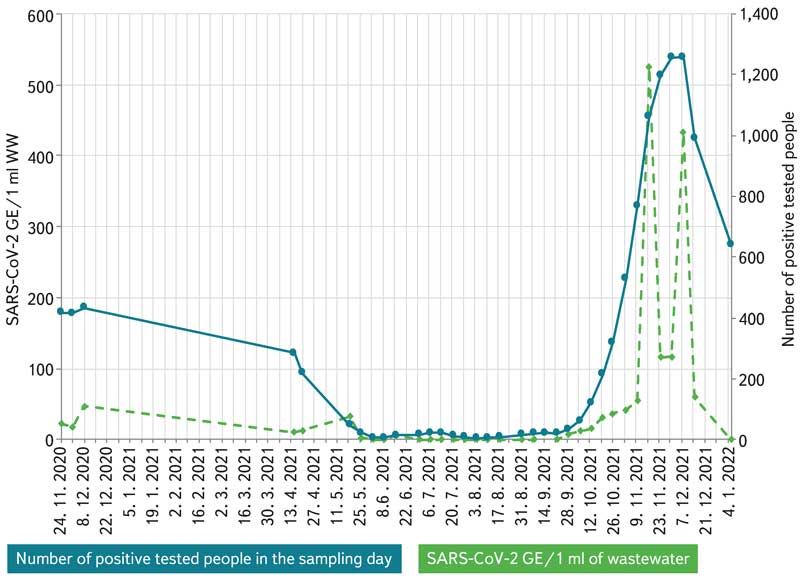
Fig. 5. Comparison of numbers of positive tested persons and amount of GE SARS-CoV-2 in wastewater from Kladno WWTP (80,000 connected people)
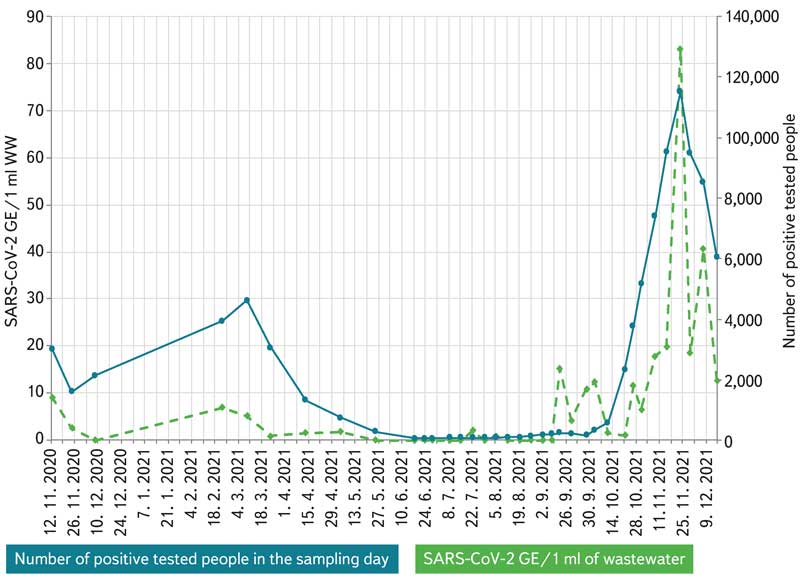
Fig. 6. Comparison of numbers of positive tested persons and amount of GE SARS-CoV-2 in wastewater from Brno WWTP (626,000 connected people)
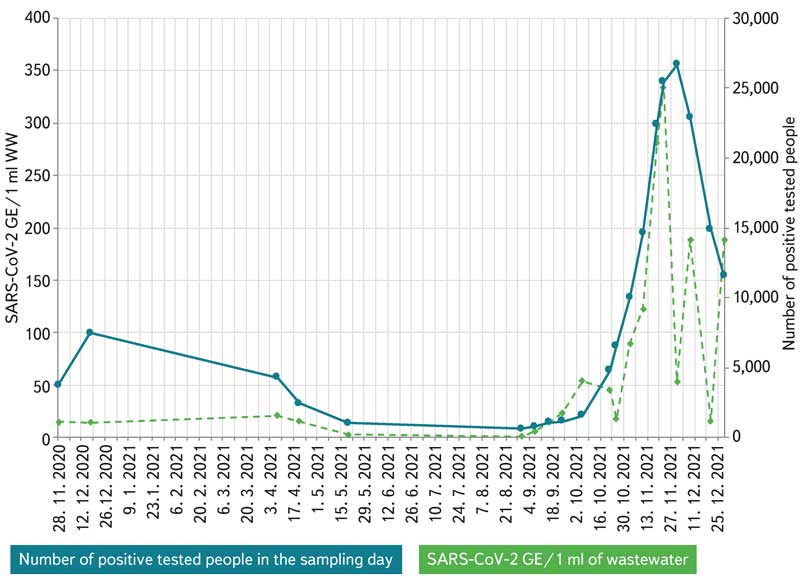
Fig. 7. Comparison of numbers of positive tested persons and amount of GE SARS-CoV-2 in wastewater from the new water line of Praha WWTP (about 600,000 connected people)
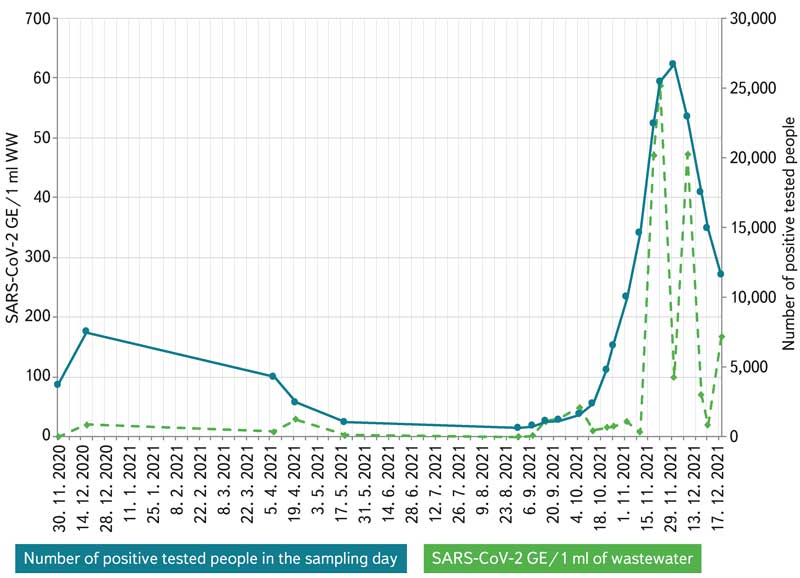
Fig. 8. Comparison of numbers of positive tested persons and amount of GE SARS-CoV-2 in wastewater from the current water line of Praha WWTP (about 600,000 connected people)
The smallest of the evaluated treatment plants was the Buchlovice WWTP, to which 2,340 inhabitants are connected; the capacity corresponds to 2,756 population equivalent (PE) The WWTP was monitored in the autumn of 2020 and in the spring of 2021. The inflow of wastewater ranged from 570 to 700 m3/day.
From the category up to 10,000 PE, the Slavkov u Brna WWTP was monitored, to which 6,500 inhabitants are connected; the capacity corresponds to 9,451 PE. The WWTP was monitored in autumn 2020 and spring 2021. The inflow of wastewater ranged from 1,200 to 4,000 m3/day.
From the category of 10,000–100,000 PE, the Tišnov WWTP was monitored, to which 11,440 inhabitants are connected; the capacity corresponds to 18,000 PE. The WWTP was monitored in autumn 2020 and spring 2021. The inflow of wastewater ranged from 2,400 to 5,100 m3/day.
Another treatment plant in the category of 10,000–100,000 PE was the Přerov WWTP, to which 41,440 inhabitants are connected and whose capacity corresponds to 112,170 PE; it was monitored in autumn 2020 and spring 2021. The inflow of wastewater ranged from 9,980 to 16,700 m3/day.
The last selected treatment plant from the category of 10,000–100,000 PE was monitored in Kladno-Vrapice. 80,000 inhabitants are connected to this WWTP, the capacity corresponds to 85,000 PE. Monitoring took place in the autumn 2020 and from April 2021 to January 2022. The inflow of wastewater in this period ranged from 8,300 to 14,000 m3/day.
The WWTP from the category of over 100,000 PE was represented by the Brno (Modřice) WWTP. 426,500 inhabitants are connected to this WWTP, the capacity corresponds to 640,000 PE. The WWTP was monitored from autumn 2020 to January 2022. The inflow of wastewater in the monitored periods ranged from 64,000 to 250,000 m3/day.
The monitored treatment plants also included Prague CWWTP, consisting of two water lines – new (NWL) and existing (EWL). A total of 1,297,000 inhabitants of Prague (1,746,500 PE) are connected to the WWTP, with each of the two water lines serving about half of them. Prague CWWTP was monitored in autumn 2020, spring 2021, and from August 2021 to January 2022. The inflow of wastewater ranged from 81,200 to 215,000 m3/day.
The interim results of the study presented in the figures show a good correlation between the amount of viral RNA in wastewater and the number of people tested positive (people tested positive in the figures are counted from day 10 before the date of the first symptoms to day 3 after the positive PCR test). Copying the trend of both curves is evident in all size categories of WWTP, while the value of reliability is up to 0.9. The presented results are gradually refined by supplementing epidemiological data and the results of other analysed frozen samples. Although the available data do not show a direct relationship between the number of infected people and the number of GE SARS-CoV-2 in the wastewater for selected WWTP, they demonstrably show the trends in the number of positively tested people and are, therefore, useful for estimating prevalence based on comparisons with previous waves of the epidemic (Fig. 1–8).
The sensitivity of the method depends on a group of factors that affect the character of the wastewater, i. e.:
- the current amount of wastewater that will affect the dilution of viral RNA in the sample,
- current share of industrial wastewater, rainwater, and municipal wastewater,
- representativeness and homogeneity of the sample,
- weekly sampling regime (differences within working days/weekends),
- length and branching of the sewerage network (RNA degradation before inflow to the WWTP, including the effect of temperature and pH of water in the sewerage system).
The correlation of both groups of data is also influenced by the robustness of epidemiological data, which are affected by the current epidemic regime. It determines the number of people who are tested, based on the frequency and method of testing, the mobility of people, the number of tests performed, etc. Another factor is the hitherto insufficient information on the proportion of people excreted viruses by the digestive or urinary tract and on the contribution from asymptomatic individuals.
It is often very difficult to estimate the amount of a virus in raw wastewater due to the lack of information on hourly and even seasonal changes in the number of viral agents in wastewater. Sampling of composite hourly samples from the Brno WWTP, which was carried out in October 2021, showed the time periods in which the largest amount of viral RNA was detected in the inflow to the WWTP (Fig. 9). The results of time monitoring of SARS-CoV-2 RNA demonstrated the possibility of effective use of an abbreviated sampling regime (e. g. between 5 a. m. and 11 p. m.), especially if it is necessary to obtain samples with higher concentrations of viral RNA for sequencing purposes. If it is not possible to provide 24-hour composite samples for analysis and it is necessary to proceed with grab sampling, sampling at times when the faecal load is highest is preferred.
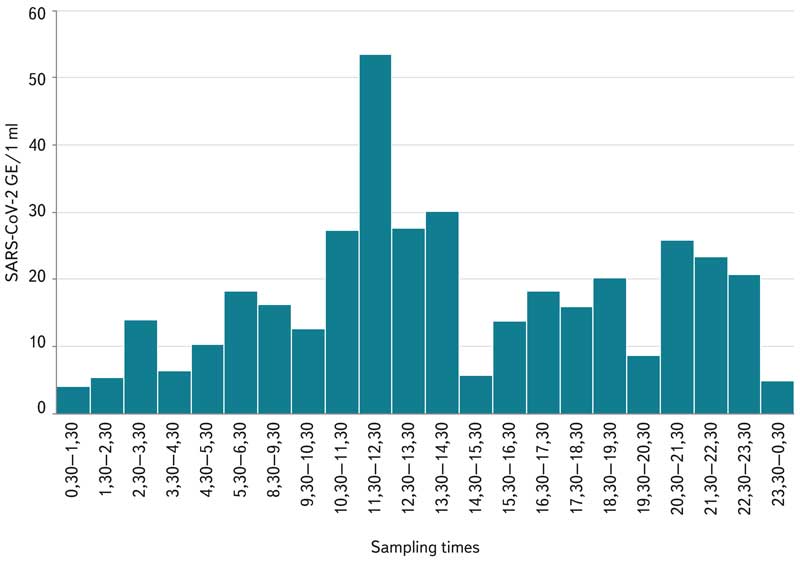
Fig. 9. Comparison of the amount of GE SARS-CoV-2 in wastewater from Brno WWTP at hourly intervals during 24 hours (11 October 2021)
The high sensitivity of the method is evident from the finding that in the wastewater of smaller WWTP, there was a positive detection of viral RNA for units of up to dozens of people detected by clinical PCR testing (e. g., Buchlovice 12 people; Slavkov 9 people; Tišnov 3 people); tens to hundreds of positively tested people were detected at larger WWTP (Brno 86 people; Kladno 14 people; Přerov 131 people). In Prague CWWTP, which was monitored only in periods with a higher prevalence, a positive RNA finding was recorded for > 600 people. The results reflect the factor of dilution of wastewater with rainwater and industrial wastewater, which must be taken into account when interpreting the data correctly.
The results of the study correspond with the findings of researchers in other countries where WBE monitoring of SARS-CoV-2 is actively underway to expand the possibilities for effective measures to combat the spread of infectious diseases. Monitoring in the world is primarily targeted on large WWTP [6]. However, in many countries, smaller WWTP, city districts, or individual buildings are also monitored [7, 8].
In some countries, the WBE approach is already applied in practice; for example, at university dormitories in Carolina (USA), asymptomatic infected students were found who would not otherwise be detected. In the Netherlands, health professionals use wastewater data to determine where to send their mobile test buses. In Australia, where the number of cases was relatively low, wastewater monitoring helped reassure authorities that their pandemic surveillance is working [9].
When considering the potential limitations of WBE for SARS-CoV-2 surveillance in the studied population, it is important to consider a number of variables that determine the quantitative ability of WBE to determine the relationship between viral RNA levels in wastewater and the incidence of infection in the population. A major constraint on SARS-CoV-2 estimation in the community using WBE is the lack of reliable data on the rate of faecal and urinary excretion of virus RNA into wastewater. For asymptomatic individuals, the rate of virus excretion is typically much lower than in symptomatic patients. In addition, there are several variables that affect the rate of excretion, including the duration of infection, levels of viremia, age of the patient, in addition to the stage and severity of the disease. A combination of WBE approach with clinical testing data in public health decision making appears to be useful [10, 11].
Another thing to consider when using WBE for Covid-19 surveillance in population is ethical aspects, as WBE does not provide data regarding the individual. In order to assess the infection spread, ideally, smaller subpopulations are monitored to define the outbreak area. This raises some ethical questions, as these areas may be subject to changes introduced by local public health authorities, which may lead to stigmatization in the behaviour of the local population, such as increased activity by people who do not want to be vaccinated [10–12].
The reliability of WBE approach depends on the lowest possible load of viral RNA that can be detected in wastewater. This value is again determined by a number of variables, including the structure of the local sewerage network, the size of the sampling area, the excretion of individuals, and viral RNA quantification methods and back-calculation models [10, 11].
Another potential limitation when considering WBE approach is the ability of the public health service to respond to the findings. Although virus detection is accurate, if data is not delivered to public health authorities in a timely manner and is not used in a timely manner, it is ineffective. In addition, there may be areas where SARS-CoV-2 in faeces can be detected consistently, so these areas need to be closely monitored due to the sudden increase in viral RNA in wastewater [13–15]. Early detection of the presence of SARS-CoV-2 in communities can also give health authorities time to prepare for potential outbreaks and ensure that adequate medical supplies, including ventilators, ICU beds, and operating staff, are available in correlation with the level of risk [16].
CONCLUSION
Monitoring of viruses in wastewater is currently used as an early epidemic warning tool in many countries around the world, with some of them systematically at the level of national programmes. Based on the Recommendation of the European Commission on the introduction of systematic monitoring of SARS-CoV-2 in wastewater of 17 March 2021 [17], which is obligatory for all member states, the Czech Republic will participate in monitoring wastewater from WWTP in towns with more than 150,000 inhabitants.
The results of our research and the conclusions of many ongoing studies clearly show that in its targeted and systematic implementation, wastewater diagnostics can be a suitable approach to the formulation of epidemiological prognoses, and thus the protection of public health. Wastewater monitoring is a sensitive method that can be used at WWTP of various sizes, even with a low prevalence of infected people in the catchment area. In Prague, the functionality of the approach was proven for smaller urban areas and individual buildings (e. g. schools and retirement homes). By adjusting the sampling time, we demonstrated the possibility of increasing the recovery of viral RNA from wastewater samples. For responsible implementation of WBE monitoring, it is necessary to accept differences between the types and purposes of monitoring, the nature of wastewater, and the specifics of sampling points.
Acknowledgments
This paper was created with the support of the project VI04000017 “Use of wastewater monitoring as an early warning tool against the emergence of the epidemiological situation” of the 4. VS BV III programme and institutional resources of the Ministry of the Environment. The authors thank the WWTP operators for their helpful cooperation in providing wastewater samples and the Department of Biostatistics of the NIPH for the provided data on the number of infected people in the monitored localities.
The paper has been peer-reviewed.
